ACGME Case Log Requirements
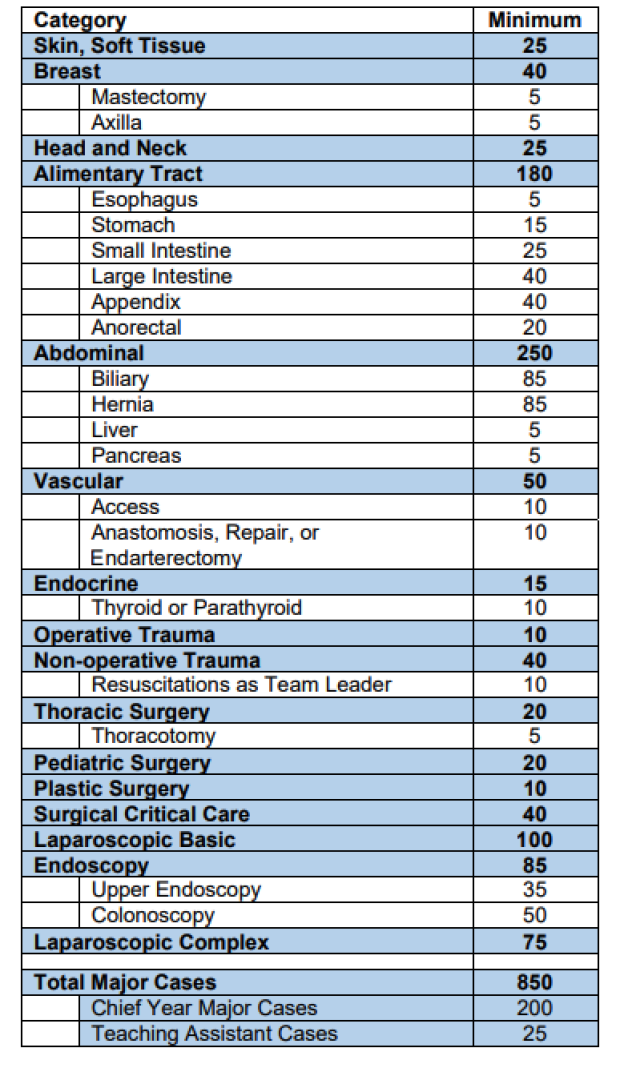
Defined category minimums, and discreet cases within each category, are in effect for residents graduating in 2018. Beginning with the January 2020 ACGME annual program review, the Review Committee will use these defined minimums to assess graduate Case Logs.
The statistical reports for graduates in the specialties listed above have been made public by the Review Committee and are also available in the ACGME Accreditation Data System (ADS).
ABS Case Log Requirements
For specific inquiries regarding ABS training requirements, please send an email to the ABS coordinator.
Residents must function in the role of Surgeon for a minimum of 850 operative procedures over the five years of residency. Of these 850, at least 200 must be accomplished as a Chief Resident.
A resident is considered the Surgeon only when he or she can document a significant role in the following aspects of management:
For multi-procedure operations, residents must record all procedures performed and indicate which procedure will count as the primary procedure. When more than one resident is involved in the same patient/same day/same operation/procedure, a senior resident may take credit as Surgeon, while another resident may take credit as First Assistant; or, a senior resident may take credit as Teaching Assistant while a more junior resident takes credit as Surgeon Junior. If two residents perform different procedures on the same patient (different CPT codes), then each may take credit as Surgeon.
SC = Surgeon Chief: Used for cases credited as “Surgeon” during the 12 months of Chief experience
SJ = Surgeon Junior: Used for cases credited as “Surgeon prior” to Chief experience
TA = Teaching Assistant: Used when a Chief Resident is working with a junior resident who takes credit as “Surgeon Junior”
The minimum required number of TA cases may be reported during the PG-4 and 5 years. All TA cases will count toward the total major cases, and will coun in the defined categories, but will not count toward the 200 minimum cases needed to fulfill the operative requirements for the Chief year.
FA = First Assistant: Used when a resident assists another surgeon with an operative procedure and when he or she is not the primary
SICU & Trauma Cases Requirements
These cases must be logged into the ACGME case log system, just like an operation. For the rising 4s, if you haven't done it yet, then I suggest you go back through your ICU time soon and log those cases before you can't find them.
Major traumas when you lead resuscitation
Select CPT Code 92950
Critical Care Index LOG Reports
Select CPT Code #99292
Critical Care Cases
For your Residency training, the ACGME requires you to do at least 40 Critical Care index cases (CPT code 99292). Within this code category you will be prompted to select an RRC code to map to the 99292 CPT code. You should have at least 2 RRC codes selected per patient out of the seven available categories. Detailed information regarding critical care guidelines can be found under the 'procedure tab' after you log into the ACGME database.
Critical Care Case Log Guidelines
The system will allow residents to identify the required minimum 40 surgical critical care index cases by using CPT Code 99292. Code 99292 will map to all seven of the surgical critical care conditions.
It is important for new users entering CPT code 99292 to understand that this index category is different from the other codes. CPT code 99292 (and it alone) will allow credit to be taken for multiple procedures on the same patient on the same day.
Reports will provide both a summary of all instances in which the resident managed 2 of the seven index critical care conditions and a detailed report for each patient encounter that will identify all the 7 conditions that were managed by the resident for any one patient.
RRC Code Assignment to New Surgical Critical Care Procedures
Following is a list of RRC procedure values that have been assigned to the newly developed Surgical Critical Care Patient Management Procedures:
8410 - Ventilatory Management (>24 hrs on ventilator)
8420 - Bleeding (non-trauma patient >3 units)
8430 - Hemodynamic instability (Req. Inotropic/pressor support)
8440- Organ dysfunction (renal, hepatic, cardiac failure)
8450 - Dysrhythmias (requiring drug management)
8460 - Invasive line management/monitoring (Swan-Ganz, catheter, arterial lines, etc)
8470 - Parenteral/enteral nutrition
Trauma & NON-Operative Trauma Cases
Log Non-Operative Trauma Cases: Select CPT Code # 99199
For your Residency training, the ACGME requires you to do at least 40 Trauma Non-operative management Cases
The category, major organ trauma, no operation required (MOTNOR), is defined as patients with major organ trauma who were admitted to a specialty care unit in the hospital, i.e., SICU, Burn Unit, T/NICU. If the patient subsequently requires a general surgery operative procedure (thoractomy, laparotomy) that may be claimed in the defined category, “Trauma, operative,” this case should be recorded using an operative code and not as MOTNOR.
Guidelines include:
The most senior resident on the trauma service should claim credit for the non-operative management
If the patient subsequently requires a general surgery operative procedure that may be claimed in the defined category, "Trauma, operative," then this case should be recorded as "Trauma," and not as non-operative management.
The category, major organ trauma, no operation required (MOTNOR), is defined as patients with major organ trauma who were admitted to a specialty care unit in the hospital, i.e., SICU, Burn Unit, T/NICU. ▪ The most senior resident on the trauma service should claim credit for the MOTNOR cases. The CPT code is 99199. ▪ If the patient subsequently requires a general surgery operative procedure that may be claimed in the defined category, “Trauma, operative,” this case should be recorded using an operative code and not as MOTNOR.